 Integrating tobacco cessation into primary care is overlooked in many countries, highlighting a need to develop suitable interventions. Dr Sushil Baral, Managing Director of HERD International, reports on the recent regional workshop for capacity building in tobacco cessation organised by the World Health Organization South East Asia Region in New Delhi, India.
Integrating tobacco cessation into primary care is overlooked in many countries, highlighting a need to develop suitable interventions. Dr Sushil Baral, Managing Director of HERD International, reports on the recent regional workshop for capacity building in tobacco cessation organised by the World Health Organization South East Asia Region in New Delhi, India.
Action plans for the development and implementation of locally appropriate tobacco cessation models in primary health care have been drawn up by the member states of the World Health Organization South East Asia Region (WHO SEAR). These include establishing quit-line services, introducing behaviour change approaches, and integrating tobacco cessation in routine primary health care settings.
A regional workshop organised by WHO SEARO on 23-24 April in New Delhi, India saw participants from all WHO SEARO member states and Cambodia (WHO Western Pacific Region) discuss the implementation of Article 14 of the WHO Framework Convention on Tobacco Control (WHO FCTC) and the WHO MPOWER technical package for tobacco cessation.
Article 14 requires parties of the Convention to design and implement effective programmes aimed at promoting the cessation of tobacco use. This includes developing and disseminating appropriate, comprehensive and integrated guidelines based on scientific evidence and best practices, taking into account national context and priorities, and taking effective measures to promote cessation of tobacco use and adequate treatment for tobacco dependence. The WHO MPOWER (Monitor, Protect, Offer, Warn, Enforce and Raise) package is a tool used to assist countries with WHO demand reduction tobacco control measures.
The “O” of MPOWER refers specifically to “Offering Help” to tobacco users to quit smoking. However, many countries in the South East Asia Region (SEAR) are struggling to find appropriate mechanisms to help tobacco users quit.
Nepal has the third highest number of young female tobacco users in the SEAR, while the percentage of young male tobacco users ranks fifth. The percentage of male (fifth) and female (fourth) tobacco users overall is also significant. While Nepal has made notable progress in introducing tobacco control related acts and policies in recent years, their effective implementation remains challenging. This includes support mechanisms for tobacco cessation.
A study conducted by the Health Research and Social Development Forum (HERD)/HERD International, Nepal in collaboration with the Nuffield Centre for International Health and Development, University of Leeds, UK in two primary health care centres in two districts of Nepal, showed 37% of smokers who received a behavioural support intervention to promote tobacco cessation were able to quit smoking. The study was funded by UKAid under the COMDIS HSD research programme consortium.
Though the study highlighted a few limitations, the findings were clear enough to say that strengthening tobacco cessation in primary health care is the best way of “Offering Help” to tobacco users trying to quit.
“To reach out to the large number of people who require support, we need to promote integrated partnership at the primary health care level,” said Dr Dongbo Fu of WHO FCTC. “It could be programmes related to tuberculosis, oral health, maternal and child health, or non-communicable diseases like the package of essential non-communicable (PEN) disease interventions.
“If every primary care provider is able to give certified advice as part of their routine practice, we will be able to reach large numbers of tuberculosis patients. As this is an opportunity that they come to primary care level for other health problems,” he added.
To provide support at the primary care level, suitable interventions need to be designed, healthcare providers need to be trained on how to use the interventions and supportive supervision is needed for the successful implementation of the interventions. This requires investment and political commitment.
Dr Jagdish Kaur of WHO SEARO said: “Basically, tobacco cessation has to be a priority. There has to be political commitment, resources to meet their action plan and international cooperation and coordination among the partners and stakeholders. I think these are the important key issues.”
Dr Tibor Szilagyi of WHO FCTC said: “Countries should come up with the plan to ensure that such resources are available. Of course there are international donors and assistance can always be found, but in some cases this might be difficult. So to start, every partner to the convention should think about how to ensure the necessary resources for its programmes.
“Tobacco taxation is a very good example, because taxing a product that kills every second consumer is a very good step. There is a need for advocacy with the Ministry of Finance that tobacco control is an intervention worth financing with more resources. It’s relatively easy to argue that part of the state income generated by tobacco taxation should be turned back into tobacco control programmes,” he added.
Category Archives: Uncategorized
Is open access really open for researchers in the Global South?

In this blog post, COMDIS-HSD Research Communications and Uptake Manager, Nilam Ashra-McGrath, reflects on the challenges of open access in the Global South.
The academic publishing industry has a global footprint, but how much of what it produces – research articles, books, conference papers – is actually accessible to those outside of academia, particularly researchers who choose to use their skills in other sectors, and the communities and citizens that research claims to benefit?
At COMDIS-HSD, I have the unique vantage point of being based within an academic institution in the UK (University of Leeds), yet work exclusively with NGOs in the Global South. From this vantage point, I can see there is an enormous imbalance in how evidence is accessed depending on whether a researcher is based inside or outside an academic institution – a symptom of an imbalance of power between the Global North and South.
Researchers who are based at academic institutions enjoy privileged access, whilst researchers who choose to work in other sectors (NGOs, media outlets, charities, businesses) face barriers that they would not ordinarily encounter if they had remained in an academic institution. Having experienced first-hand the effect this has had on our consortium of NGOs, I believe there are two changes that universities, academic publishers and access schemes like Research4Life could do to help address this imbalance.
The first is to give researchers working outside academia the same status and privileges as those working in universities. Evidence is the lifeblood of any researcher and any barriers to accessing evidence cuts off their blood supply. It also has a negative impact on the capacity of researchers in low and middle income countries (LMICs) to do their job effectively. By contrast, easy access to evidence gives them life, and sustains their career well beyond the walls of academia, irrespective of the sector in which they choose to work. Qualified researchers therefore need access to the same information and privileges they had when they were training in the UK; this is fundamental to them being able to earn a living as a researcher.
The second is to ensure that access rights follow the migratory pattern of researchers into different organisations and sectors throughout the lifetime of their careers. The Royal Society highlighted that 42% of postgrad researchers in the UK are international. Many are from LMICs. When they receive training in the UK (and North America and Europe for that matter), they have an infrastructure around them to help access and share research findings, to design and implement research based on what has come before, and to add to an existing body of knowledge.
When they return home, it’s not uncommon that, when faced with a dearth of university based jobs, they look to other sectors to use their research skills. This includes, but is not limited to, working for government ministries, NGOs and civil society organisations, international aid agencies, businesses, media outlets, or even as independent researchers. As qualified researchers, their skills are highly valued by other sectors. However, the infrastructure that they were once able to make use of while training in the UK is now absent, meaning that they now have to rely on significantly smaller amounts of literature to conduct research.
One way to ensure that researchers have continued free and easy access throughout their career, is for universities to allow postdocs to keep their university email address and associated library access as alumni. Some universities already offer this, but it comes with limited access to journals. Granting all postdocs lifetime access to research evidence via their former universities is either a staggeringly simple solution, or a political and resource intensive minefield (I’m guessing the latter). Nevertheless, it’s an idea that needs exploring as at the moment, it’s only the academic setting that allows researchers to do their jobs effectively.
What we need is a system that gives equal access rights and privileges for all researchers, irrespective of where they career takes them. This would be a positive step in helping researchers in LMICs flourish without relying on Northern institutions and schemes to access research evidence.
Voices from the NGO community have been on the periphery of the open access debate. With the academic publishing industry experiencing an unprecedented level of disruption, the time is right for the peripheral voices to be heard.
This article represents the views of the author, and not the position of the Department for International Development, or of the University of Leeds.
Commonwealth leaders commit to halving malaria cases in 5 years
 Leaders of the 53 commonwealth countries have committed to halving the number of cases of malaria in their countries by 2023.
Leaders of the 53 commonwealth countries have committed to halving the number of cases of malaria in their countries by 2023.
If achieved, this will result in 650,000 lives saved and prevent 350 million cases of malaria.
The announcement was made at the Malaria Summit London, held during the Commonwealth Heads of Government Meeting, where £2.9 billion ($4.1 billion) was pledged to tackle the disease. Co-hosted by the Governments of Rwanda, Swaziland and the United Kingdom, key speakers included His Royal Highness the Prince of Wales, Bill Gates, and the Director General of the World Health Organization, Dr Tedros Adhanom Ghebreyesus.
Delegates were made up of leaders from 19 Commonwealth countries, scientists, heads of business and civil society advocates.
Leaders also urged that efforts should be accelerated to reduce malaria globally by 90% by 2030.
Malaria affects 90% of citizens living in commonwealth countries and accounts for half of all global cases and deaths from malaria. In 2016, 46% of global malaria deaths occurred in eight Commonwealth countries, half of which were in Nigeria.
Speaking after the summit, Charles Nelson, chief executive of Malaria Consortium, said:
“The commitments announced today represent an important step towards mobilising the resources we need to drive progress against malaria.
“As well as increasing investments for malaria, both across the Commonwealth and beyond, we also need a smarter, more targeted approach to how we fight the disease. By investing in disease surveillance systems and strengthening the collection, analysis and use of data, malaria interventions can be more targeted, outbreak responses can be more rapid, and as a result, the impact of our work can be much greater.”
Our Malaria research
COMDIS-HSD has been involved in a number of malaria projects in commonwealth countries.
Our study with the Centre for Global Health Research in Ghana looked at the use of Intermittent Preventative Treatment in children in an area with a long malaria transmission season, and evaluated the use of a longer acting antimalarial for treatment as a means of chemoprevention.
It revealed convenient access to seasonal malaria chemoprevention (SMC) drugs, including door-to-door delivery by trusted community health workers, makes SMC more acceptable to caregivers and leads to better adherence. By extending SMC from the usual 3 months to 5 months, it can significantly reduce the burden of malaria in areas with longer rainy seasons.
Read our research brief on extended seasonal malaria chemoprevention in Ghana.
Watch our video brief on seasonal malaria chemoprevention in children under 5 years.
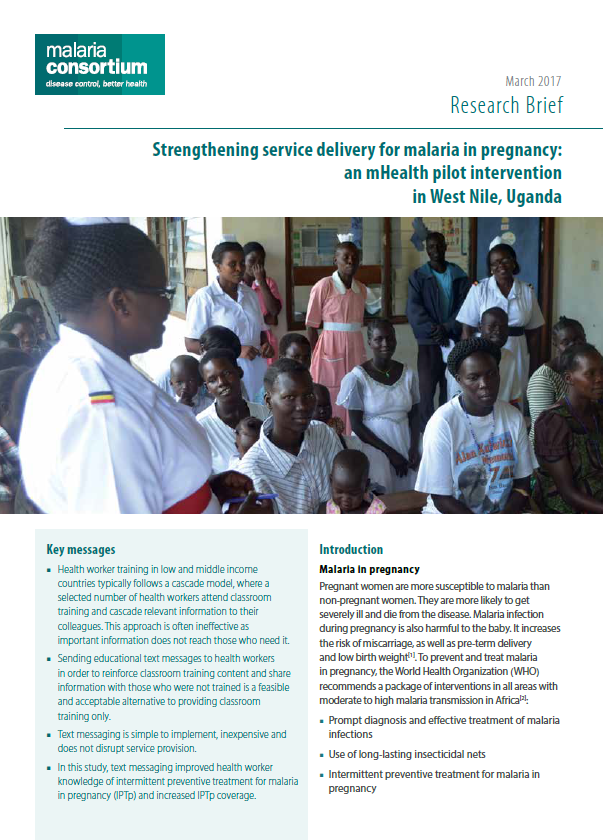
Working with Malaria Consortium, our study in Uganda aimed to increase the uptake of intermittent preventive treatment for malaria in pregnancy (IPTp).
It revealed that text messaging improved health worker knowledge of IPTp and increased IPTp coverage. As a result, the Ministry of Health in Uganda adopted a text messaging approach for health worker education and learning in its national malaria in pregnancy training strategy.
Read our research brief on introducing an mHealth pilot intervention in West Nile, Uganda.
As part of the same project, we identified barriers to two-dose intermittent preventive treatment (IPT2) in pregnancy in Uganda, offering a number of key recommendations, including the development of a job aid for health workers and the introduction of computerised recording and reporting systems at health facilities.
Read our research brief on assessing and addressing barriers to IPT2 uptake in Uganda.
{kind=link}
Universal health coverage in Bangladesh hindered by communicable and non-communicable diseases

From left: Dr Khaleda Islam, Dr Md Zakir Hussain, Mr Md Ashadul Islam, Dr Shelina Ahmed, Dr Syed Abdul Hamid
The rising burden of communicable and non-communicable diseases is preventing universal health coverage in Bangladesh, the Director General (Additional Secretary) of the Health Economics Unit, Ministry of Health and Family Welfare (MOHFW), has said.
Speaking at a health policy event in Dhaka organised by MOHFW and ARK Foundation, Dr Md Zakir Hussain said constrained resources and increasing demand are making the delivery of safe, high-quality services for the entire population challenging.
“Resources are limited, so we need to consider how we can provide services more efficiently,” he said. “We also know that we need to ensure our health services are of high quality, with patient safety at their core; and we need to consider new and innovative ways to deliver services to citizens in their homes and communities.”
The event assessed the present state of health service delivery in Bangladesh. It saw senior level policy makers, service delivery personnel, development partners, academics and researchers come together to consider future options for achieving universal health coverage.
The double burden of communicable and non-communicable diseases was also emphasised in a keynote delivered by Dr Rumana Huque, Executive Director of ARK Foundation. Presenting lessons learned from studies undertaken by COMDIS-HSD, she said training of community health care providers on integrated management of childhood illness helped them to appropriately diagnose and refer selected infectious diseases, and developed their skill in rational use of drugs, including antibiotics.
Insufficient funding was revealed as one of the biggest issues affecting successful health care delivery within the country. Dr Shelina Ahmed, Health Advisor for the UK’s Department of International Development in Bangladesh, said underspend in budgets allocated for the health sector remains a problem. She called for the need to develop institutional capacity to ensure sustainability of investment.
Dr Syed Abdul Hamid, Chairman of the Institute of Health Economics at Dhaka University, highlighted current expenditure for basic health care is almost 50% lower than the minimum requirement. Around US$ 65 is needed per person each year for basic health care services in Bangladesh, yet current spending is only $US 37 per person.
Referring to work undertaken by COMDIS-HSD, Dr Khaleda Islam, Director of Primary Health Care, Directorate General of Health Services, said improving health service delivery in Bangladesh requires facility readiness, referral and transport, routine data and monitoring, quality improvement, capacity building and retention, and social and behavioural change communication.
Mr Md Ashadul Islam, Secretary (In-Charge), Bangladesh Karmachari Kallyan Board, Ministry of Public Administration, said that service coverage should be expanded, along with increased resources that are used efficiently. He emphasised the importance of ensuring coordination across operational plans of the MOHW, and coordination among stakeholders in improving health service delivery.
World TB Day 2018: Leading the fight against TB

The University of Leeds and Leeds City Council organised key landmarks to be illuminated red to promote awareness of the global burden of TB
COMDIS-HSD partners led the way in international events for World Tuberculosis (TB) Day on 24 March. Activities were organised across the globe to promote awareness of the disease under the theme “Wanted: Leaders for a TB-Free World”. The World Health Organization called on anyone affected by the disease to come forward as leaders in the fight against TB. Alongside heads of state and political leaders, this included doctors, health workers, patients and families.
COMDIS-HSD: Lighting the town red against TB
The University of Leeds and Leeds City Council organised public buildings to be illuminated as part of a Stop TB global initiative to light up key landmarks. The town hall, civic hall and university’s Parkinson building were all lit up red to show commitment to tackling TB.
Academics from COMDIS-HSD were also involved in a joint letter sent to UK Prime Minister, Theresa May, urging for more action against TB.
James Newell, Professor of International Health at the University of Leeds, said:
“TB continues to be the top infectious killer worldwide, claiming over 4,500 lives a day. Increasing rates of TB resistant to the drugs commonly used for treatment – so-called multidrug-resistant TB – poses a major global health threat and threatens gains made in the fight against the disease.
“Because TB and multidrug-resistant TB are spread from one person to another through droplets in the air, they pose a threat to everyone in the world, not just people in developing countries: in fact, rates of TB are higher in some areas of the UK than in parts of Africa and Asia.”
Helen Elsey, Associate Professor in Public Health at the University of Leeds, said:
“TB is still an important health issue in Leeds, affecting some of our most vulnerable communities, with 425 new cases in 2016 in Yorkshire and Humber.
“The most significant impacts of TB are seen in low income countries, where 95% of cases and deaths occur. The global community has set a goal to end the TB pandemic by 2030.
“However, a recent World Health Organization report warned that current global actions and investments fall far short of those needed to achieve this goal. There is an urgent need to mobilise political, social and resource commitments to ensure that here in the UK and globally we can end this debilitating and dangerous disease and the human suffering which it brings.”

ARK Foundation take to the streets in their annual World TB Day rally
ARK Foundation: We have to work together to eliminate TB
ARK Foundation took to the streets of Dhaka once again for their annual World TB Day rally. Around 1500 people joined the procession led by TB leaders, which followed a route from the Bangladesh National Museum to the iconic Doel Chatar sculpture.
Dr Mozaffar Hossain Paltu, President of the National Anti-Tuberculosis Association of Bangladesh, said: “It has been more than 100 years since TB was discovered by Dr Robert Koch and we haven’t stopped it yet. We have to work together to eliminate TB from Bangladesh and the world.”
To accompany the rally, Ark Foundation produced 15,000 fact sheets circulated to hospitals, clinics and health centres nationwide. They were were also sent to administrative divisions before the event.
{kind=link}
HERD International: laying the foundations against TB
HERD International were involved in a programme organised by the National Tuberculosis Centre in Thimi, Bhaktapur.
As part of the day’s events, Minister of State for Health, Padma Kumari Aryal, laid the foundation stone for the future National Chest Disease Hospital in Bhaktapur. It is to be a specialist, tertiary referral hospital for difficult cases of TB and other respiratory diseases, and will be developed as a “centre for excellence” at the national level.
“The hospital will help to provide timely treatment to tuberculosis patients,” said Dr Kedar Narasing KC, Director of the National Tuberculosis Centre.
Featuring 300 beds, it is planned to be constructed within 3 years.
ASD: Creating awareness about TB prevention
In Pakistan, activities took place in 13 districts where ASD have been implementing public-private mix TB interventions. During March, 25 community gatherings were held to create awareness about TB prevention, alongside 25 chest camps screening individuals for TB. Seminars were held in each district with an average attendance of 50-60 people. TB awareness banners were displayed on rickshaws, with larger banners displayed in prominent places. Press briefings were held in eight districts and local cable networks broadcasted TB awareness messages for 2 weeks.
In 12 teaching/specialised hospitals, health staff gathered at Programmatic Management of Drug-Resistant TB sites to celebrate World TB Day. Where possible, walks were organised around hospital premises. Lectures were delivered by the MDR physician/professor of pulmonology at each site, outlining the prevalence of TB, transmission of the disease, diagnosis, and the free treatment provided by The Global Fund.
James Newell, COMDIS-HSD Co-Director, reflects on our impact and influence in 2017
![]()
Here at COMDIS-HSD, we’ve been reflecting on our impact and influence in 2017, which began with a 2-year extension to continue some of our work. Our review of 2017 showcases our influence and work in Bangladesh, China, Nepal, Pakistan and Swaziland – I hope you enjoy reading about some of our successes in TB, malaria, antibiotic resistance, gender and open access.
I’d also like to thank all our partners for their great work and support in developing and initiating this work, including, but not restricted to:
- international and government partners for working with us to identify research questions of global importance
- COMDIS-HSD research partners for developing and carrying out the research and working closely with government and other partners
- the team in Leeds for providing research, communication and operational support
- Consortium Advisory Group members for guidance and support
- Colleagues at DFID for providing funding and supporting us in navigating new DFID requirements.
All this input means we have been able to continue to develop and assess strategies that are designed to be appropriate for context, scalable and sustainable, and that over the years have helped improve the health of millions of people in our study countries and beyond.
![]() I am particularly excited by three new areas of work: 1) hepatitis prevention and care; 2) psychosocial support to people with MDR-TB; and 3) improving health care, particularly for communicable diseases, in urban areas. Although time is tight, we aim to deliver findings in these areas that will guide national and disease control programmes and international bodies by providing feasible and practical solutions to these major problems.
I am particularly excited by three new areas of work: 1) hepatitis prevention and care; 2) psychosocial support to people with MDR-TB; and 3) improving health care, particularly for communicable diseases, in urban areas. Although time is tight, we aim to deliver findings in these areas that will guide national and disease control programmes and international bodies by providing feasible and practical solutions to these major problems.
 I am also delighted to welcome Libby Clark, our newly appointed Consortium Manager, to the team. Libby comes to us with a wealth of programme management experience coupled with a background in gender and development – a great fit for our consortium.
I am also delighted to welcome Libby Clark, our newly appointed Consortium Manager, to the team. Libby comes to us with a wealth of programme management experience coupled with a background in gender and development – a great fit for our consortium.
I’d like to end by thanking everyone involved for their continuing support. We look forward to reporting on our impact in these areas of work in 2018.
How our research has helped reduce unnecessary antibiotic prescribing for children in China
![]()
This news story was first published on the University of Leeds health news pages. It describes our work at COMDIS-HSD to combat the inappropriate use of antibiotics – a major global risk factor in the development of drug-resistant ‘superbugs’.
A collaboration between scientists has helped reduce the prescription of unneeded antibiotics to children in rural China.
Young people in some areas of the country are being given antibiotics, often intravenously, to treat a cold, ear or throat infections – but the drugs are not effective against virus-based illnesses.
The inappropriate use of antibiotics is a major risk factor in the development of drug-resistant “superbugs”.
Antibiotic use halved
The collaboration brought together rural hospitals in two counties in rural China, Chinese health officials and academics at the University of Leeds (COMDIS-HSD) and the University of Toronto.
The aim was to devise and evaluate a system of ‘anti-microbial stewardship’ that could be used in other parts of the Chinese health system and would give doctors the confidence to say no to requests for inappropriate antibiotic treatment.
The stewardship programme was rolled out to a group of primary care hospitals in Guangxi province in Southern China.
Much of the demand for antibiotics in the Chinese primary care sector comes from parents and grandparents who have children with upper respiratory tract infections such as a sore throat or earache.
Doctors working in the primary care hospitals come under considerable pressure from parents to prescribe antibiotics to children who have upper respiratory tract infections
John Walley, Professor of International Public Health at the University of Leeds, said:
“Doctors working in the primary care hospitals come under considerable pressure from parents to prescribe antibiotics to children who have upper respiratory tract infections.
“They can feel that if they don’t give the antibiotic, the parents will just go elsewhere and get it.
“These are difficult decisions for the doctor. They may have a very ill child in front of them – and they do not have a battery of tests results to rely on. They are having to make a clinical judgement about the risks involved in not giving antibiotics.”
New guidelines for doctors
University academics and Chinese experts drew up clinical guidelines based on those produced by the UK’s National Institute for Health and Care Excellence to help doctors decide when it would be appropriate to prescribe antibiotics and alert them to the warning signs of more serious illness.
Two groups of primary-care hospitals in Guangxi were selected for the evaluation. Baseline data was collected about the prescribing practices for children attending with upper respiratory tract infections.
In the first group, containing 12 hospitals, doctors received training in how to explain to parents why antibiotics are not necessary. Medical managers also conducted monthly prescription reviews to monitor doctors’ compliance with the guidelines.
In the second group, made up of 13 hospitals, medical staff continued to prescribe in the usual way.
The results showed that in the group that had received stewardship training, the antibiotic prescription rate had dropped from 82 per cent to 40 per cent
Six months later, several thousand prescriptions were selected at random from the two groups and compared with the baseline findings. The results showed that in the group that had received stewardship training, the antibiotic prescription rate had dropped from 82 per cent to 40 per cent. In the business-as-usual group, the rate went from 75 per cent to 70 per cent.
The findings were reported in Lancet Global Health.
Taking account of statistical issues, the researchers say the stewardship programme resulted in a 48 per cent reduction in the prescribing rate of antibiotics for children with upper respiratory tract infections.
Professor Walley said: “There have been other approaches that have tried to change the behaviour of doctors and patients – but none has delivered the scale of change that we have seen.”
Typically in successful trials the change is between five and 25 per cent.
The Chinese Health Ministry has policies to reduce antibiotic use but the challenge is to get that aim delivered in primary care clinics and hospitals, Professor Walley said.
He said the key to success was to “embed” stewardship programmes within the health system, giving doctors the skills and encouragement to give antibiotics when there is a real clinical need – and to refuse them when their use would be inappropriate.
The problem of the overuse of antibiotics exists in many low and middle income countries, and existed in the UK – although healthcare policies in recent decades have resulted in more careful use of antibiotics.
Read more:
- See our full research findings: Wei X, Zhang Z, Walley J, Hicks J P, Zeng J, Deng S, et al. (2017) Effect of a training and educational intervention for physicians and caregivers on antibiotic prescribing for upper respiratory tract infections in children at primary care facilities in rural China: a cluster randomised controlled trial. The Lancet Global Health. DOI
- Read our policy brief for a summary of our findings and key recommendations and see our research brief for further details on our study methods.
Read our latest e-news: Open Access Week special edition
 It’s Open Access Week 2017 and this is our special edition open access e-news with some hand-picked tools and resources to help you share your research and access other published work.
It’s Open Access Week 2017 and this is our special edition open access e-news with some hand-picked tools and resources to help you share your research and access other published work.
BLOG: Is depression contributing to low global cure rates for multi-drug resistant TB?
This blog first appeared on the Stop TB Partnership website. Our thanks to the Partnership for their support.
Blog by Dr Helen Elsey and Ian Walker of COMDIS-HSD.
Image from a patient leaflet developed as part of the psychological support package for MDR-TB patients in Nepal. It shows a counsellor using the flipbook (also part of the package) to guide discussions with a patient and family member
A marathon no-one wants to run
It takes 2 years, 14,000 pills and 6 months of daily injections before a patient can hope to be cured of multi-drug resistant TB (MDR-TB). The drugs are powerful, toxic and can cause debilitating side-effects, including hearing loss, kidney problems, depression and psychosis.
If treatment is erratic or interrupted, it won’t work. If you are poor and live in a low-income country you are likely to have even bigger problems. Stigma and social isolation, difficulty accessing treatment centres and being unable to work are just some of the well-documented challenges patients face.
Against this backdrop, how surprising is it that only half of all people who start treatment for MDR-TB are successfully cured? The global TB community is striving to develop better, simpler and faster-acting TB drugs. The goal, says the TB Alliance, is the development of ‘relatively short course (6 months) of daily, all oral, affordable novel medications’. Few would argue with this priority. But is it the whole answer? Even with shorter 9-month treatment regimens now being rolled out in some countries, what about the significant negative effect of MDR-TB on the mental wellbeing of patients, and what impact will this continue to have on adherence and cure rates?
‘I have not seen anyone surviving’
We have learned a lot from our research in Nepal about the wider impacts of MDR-TB. Patients have told us about the guilt of becoming a burden on their families, the financial hardship and stigma, the breakdown of family relationships and, ultimately, their sense of hopelessness.
‘I think about the future. I have MDR-TB now and I think about my children. I have only seen people dying from MDR-TB. I have not seen anyone surviving.’ MDR-TB patient from our study in Nepal
We are also beginning to understand the additional gender-based inequities faced by female MDR-TB patients, particularly married women who are frequently abandoned by their husbands and struggle to look after their children and manage their illness. What we don’t yet understand is how many patients go on to have depression, when they get it and whether they are less likely to be cured as a result.
Depression and the TB timeline
The negative impact of diabetes and other long-term conditions on patients’ mental health are well evidenced. The World Health Organization (WHO) states that the prevalence of major depression is consistently higher in people affected by chronic disease and that patients with co-morbid depression are less likely to adhere to medical treatment. Yet there is still very little data available on the psychological impacts of TB and MDR-TB. Big questions remain
At COMDIS-HSD, we are working with ARK Foundation in Bangladesh to understand more about the timeline of depression for people with MDR-TB. We want to find out:
- How many patients have depression?
- When does depression start?
- Do depression levels fluctuate during the long treatment?
- At what point(s) do patients most need psychological support?
Together with our partners HERD in Nepal, we have already explored a number of psychological support interventions with patients in an effort to find which tools and methods work best in low-income settings. Strong evidence from India, as well as our own experience in Nepal, shows that Healthy Activity Programme (HAP) counselling is well received by patients and can be delivered by health workers and lay counsellors, with appropriate training and adequate investment in staff.
We have developed a desk guide, flip book and other information materials as part of a psychosocial support package for people receiving treatment for MDR-TB. These are the first resources focusing on psychological aspects of MDR-TB care in Nepal and are ready for adaptation and scale-up across MDR-TB services.
In developing interventions, however, one size rarely fits all and it is crucial to tailor approaches to reflect individual, cultural and country contexts.
Giving patients a mood tool
The HAP approach, for example, helps patients identify or re-engage with activities they enjoy, eg, visiting family, talking to friends, tending to the garden or crops. It takes a gradual, problem-solving approach. Patients work with a trained health worker or non-specialist counsellor in one-to-one sessions over several weeks. Together, they identify activities the patient previously enjoyed, what might be stopping them from doing these (eg feeling afraid to go out alone) and the steps needed to get back on track. As patients do more of what they enjoy, their mood should improve and they have learned a practical way to trigger more positive thoughts when they are feeling low.
In Nepal, and other countries where MDR-TB patients are treated almost entirely in the community, this approach could be appropriate (although we know it requires considerable extra investment in staff in an already over-stretched TB programmes). But in Bangladesh, where MDR-TB patients spend an initial 2 months as hospital in-patients, it is unlikely to work. If you are lying in a huge hospital ward with 70 strangers and undergoing intensive treatment, taking a walk, gardening or visiting family are clearly off the agenda. Other approaches are clearly needed.
There is strong global evidence, including with diabetes patients in the UK, that peer support is helpful to patients’ mental wellbeing. Other evidence points to the positive effect of cured MDR-TB patients talking to those still undergoing treatment. Group support approaches with current and cured patients may work better in a hospital setting and we will explore these options.
Stressed or depressed?
Language too is an important consideration when developing interventions. In contexts where mental ill health still carries a heavy stigma, we have tried to find different ways of asking patients about their symptoms. In South Asia, for instance, we use words like ‘stressed’ rather than ‘depressed’.
Stigma can also dictate how patients are likely to present to their health services. Global evidence suggests that patients with depression are more likely to complain of physical symptoms, such as aches, pains or headaches, rather than talk about their feelings and mood. So, again, it is important that screening tools use the right words and are designed to pick up on the sort of physical symptoms that may be indicating underlying depression and poor mental health.
Of course, achieving all of this will be challenging. In the context of communicable diseases, the primary focus is rightly on drugs and cure. Mental health in general remains a seriously underserved area in low and middle-income countries (LMICs).
In TB, however, the focus may be starting to shift. WHO guidelines are explicit about the need for patient-centred care and the importance of emotional support:
‘The provision of emotional support services to patients may increase the likelihood of therapy adherence, and the acquisition of skills to deal with stigma and discrimination. This support may be organized in the form of support groups or in one-to-one counselling by trained providers.’
Mobilising the NCD workforce
Yet how do we make that happen on the ground? TB and MDR-TB are chronic infectious diseases and the evidence is clear that once you have a chronic condition you are more likely to have depression. So rather than developing counsellors within MDR-TB services, are there other ways to enhance these skills in primary care to meet the needs of a variety of patient groups?
In our current study in Swaziland we will begin to explore this model. Working with our partners at Good Shepherd Hospital, our research will look at the feasibility of delivering psychological counselling in HIV and TB treatment. We will train non-communicable disease (NCD) nurses to deliver much of the psychological support intervention.
While the race is on to develop and implement faster, simpler and more effective medications for MDR-TB, making the case for depression screening and psychological counselling is not an easy job. But it is an important one.
Much of what we are doing on MDR-TB and depression will be hugely relevant to other chronic conditions. Across all major diseases it is important every effort is made to put mental health not just on the national political agendas for LMICs, but somewhere near the top.
- For more information contact Ian Walker at: [email protected] or Dr Helen Elsey at: [email protected]
- Or visit comdis-hsd.leeds.ac.uk
Notes on the authors:
Dr Helen Elsey is Associate Professor in Public Health at The Nuffield Centre for International Health and Development at the University of Leeds. Helen’s research interests lie in applied global public health research, particular in urban areas, developing and evaluating public health interventions that reduce risks to health and improve health behaviour.
Ian Walker is a Visiting Research Fellow and Specialty Registrar in Public Health at The Nuffield Centre for International Health and Development at the University of Leeds. A former mental health nurse, Ian has a special interest in global mental health research, particularly in the implementation of psychosocial interventions.
See also our partner HERD’s interview with Sailu Rajbhandari, a clinical psychologist in Nepal.

Clinical psychologist, Sailu Rajbhandari on mental health in Nepal: “In the recent years, there is an increased realisation among the government stakeholders on the need to tackle mental health issues. I feel that we need to sensitize our stakeholders on mental health issues. Awareness at all levels, including household level is essential”
SaveSave
SaveSave
SaveSave
SaveSave
SaveSave
SaveSave
SaveSave
SaveSave
SaveSave
SaveSave
SaveSave
COMDIS-HSD awarded £2m extension by DFID

COMDIS-HSD team members at our 2017 annual partner meeting in Kathmandu, Nepal in July
We are delighted to announce that COMDIS-HSD has been awarded a £2 million extension by the Department for International Development (DFID). This will run until December 2018. Our research will continue to focus on health service delivery for communicable diseases, and in particular on:
- tuberculosis: continuing our work to develop a psychological support package to improve the metal wellbeing of patients with depression during TB and/or HIV treatment;
- neglected tropical diseases (NTDs): developing tools and processes to help primary healthcare staff detect, manage and record NTDs;
- hepatitisː working with public hospitals in the Punjab to enhance diagnosis and treatment of hepatitis C and improve vaccination practices and coverage for hepatitis B;
- urban health: enhancing the capacity and skills of urban healthcare workers to deliver basic healthcare services to some of the poorest populations in Nepal.
We will continue to work closely with our 5 long-standing NGO partners: ARK Foundation in Bangladesh, ASD in Pakistan, HERD in Nepal, Malaria Consortium in Ethiopia and Good Shepherd Hospital in Swaziland, as well as in-country Ministries of Health and other relevant stakeholders. James Newell, Co-director of COMDIS-HSD, said: ‘The funding allows us to move forward with a number of exciting new studies, building on our growing body of evidence about what interventions and approaches work best to improve health service delivery in low- and middle-income countries.
‘We will continue to work hand-in-hand with ministries of health and national programmes using a range of methods, including our very successful embedded approach. We will also be encouraging our partners to capitalise on the considerable experience they have built up over the 11-year lifespan of COMDIS and COMDIS-HSD and collaborate even more closely to develop their new studies and share knowledge and skills.’
In the extension we are also hoping to formalise a new collaboration with fellow DFID consortium, Research in Gender and Ethics (RinGs). We will be working closely with RinGs colleagues to build gender sensitivity into our own organisational processes, as well as embedding it in our project and research design.
In particular, we will be using our research to understand more about how gender intersects with other aspects of inequity such as age, ethnicity and class.

Zunayed Al Azdi of ARK Foundation explains research uptake plans for our study into the mental health needs of patients undergoing treatment for MDR-TB in Bangladesh

Taking a stand: the COMDIS-HSD take to the floor to learn about pathways to impact in their research

Voting with our feet: a cross on the pavement serves as a handy visual aid when it comes to understanding transformative change during a session on gender and intersectionality

Tweeting every step of the way